Anti-Ceramide ScFv Prophylaxis for First Responders to a Limited Nuclear Attack
bDepartment of Epidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Center, New York, New York, USA,
cDepartment of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, New York, USA,
dThe Champalimaud Center, Lisbon, Portugal
Keywords
Abstract
Background/Aims:
After 9/11, multiple government agencies instituted programs aimed at developing medical radiation countermeasures (MRCs) for two syndromes lethal within weeks of a limited nuclear attack; the hematopoietic-acute radiation syndrome (H-ARS) and the higher-dose gastrointestinal-acute radiation syndrome (GI-ARS). While re-purposing drugs that enhance marrow repopulation treats H-ARS, no mitigator protects GI tract.Methods:
We recently reported anti-ceramide 6B5 single-chain variable fragment (scFv) pre-treatment abrogates ongoing small intestinal endothelial apoptosis to rescue Lgr5+ stem cells, preventing GI-ARS lethality in C57B/L6J mice. Here, with US Department of Defense support, we provide evidence that humanized anti-ceramide scFv (CX-01) is a promising prophylactic MRC for first responders, who risk exposure upon entering a radiation-contaminated site.Results:
CX-01, when delivered up to 90 min before irradiation, is highly-effective in preventing small intestinal endothelial apoptosis in mice and lethality in both sexes. Unexpectedly, females require an ~2-fold higher CX-01 dose than males for full protection. CX-01 is effective subcutaneously and intramuscularly, a property critical for battlefield use. Increasing the maximally-effective dose 5-fold does not extend duration of bioeffectiveness.Conclusion:
While CX-01 prevents GI-ARS lethality, structural modification to extend half-life may be necessary to optimize first responder prophylaxis.Introduction
Possibility of a radiation disaster by way of nuclear detonation, terrorist activity, or healthcare or industrial accident has long existed, however since 9/11 the perceived threat of attack using a radiation dispersal device has increased urgency for safe and effective medical radiation countermeasures (MRCs) [1-3]. The US Department of Defense has interest in developing agents which can be administered prior to exposure or soon after exposure under mass casualty conditions to protect first responders, military, and specialized technical personnel, who must enter an area affected by nuclear catastrophe [4]. Thus, novel therapeutic strategies represent an unmet need, especially for drugs specific for organs known to be at risk for potentially lethal radiation injury.
The Gastrointestinal-Acute Radiation Syndrome (GI-ARS) is a major lethal radiotoxicity that involves destruction of crypt/villus units, resulting in mucosal denudation, loss of nutrient adsorption and susceptibility to infection by resident bacterial flora. Clinically, the GI-ARS presents with anorexia, vomiting, diarrhea, dehydration, systemic infection, and in extreme cases, septic shock and death within days of exposure [5-7]. While the relevant radiation target for the GI-ARS is considered the intestinal stem cell (ISC) compartment within the crypt of Lieberkühn [8-12], no effective MRC for GI-ARS lethality is currently available as prophylaxis for ISC radiation injury. Our lab has provided evidence that in addition to direct ISC damage, ceramide-mediated vascular injury is critical for evolution of this syndrome due to formation of macrodomains on the endothelial cell surface termed ceramide-rich platforms, which transmit an apoptotic signal [13-17]. Further, we recently reported that anti-ceramide 6B5 single chain variable fragment (scFv) binds to and neutralizes the pro-apoptotic lipid ceramide on the GI endothelial cell surface, preventing endothelial cell CRP formation and abrogating apoptosis, which enhances Lgr5+ small intestinal stem cell regeneration, protecting against GI-ARS pathophysiology and lethality [18].
During radiological/nuclear incidents, the role of first responders includes securing the scene, decontaminating victims when needed, triaging and stabilizing patients, and providing treatment where appropriate [19-21]. It is thus critical that first responders be protected from radiation exposure during performance of these duties. However, numerous challenges exist in protecting first responders against inadvertent radiation exposure as many responders lack basic knowledge of mechanisms of radiation exposure and preventative measures designed to reduce exposure, potentially leading to radiation “dread”, a potential confounder of emergency response that may affect first responders’ willingness to work in areas where radioactive contamination is present. Availability of medical countermeasure prophylaxis might significantly mitigate impact of radiation dread, helping to maintain adequate radiation safety among first responders and emergency personnel, and improve their willingness to work during future radiological or nuclear events [22-24]. To date, no agent has received US FDA approval for GI-ARS as a radioprotector or radiomitigator. The current studies were designed to explore potential for anti-ceramide scFv prophylaxis of first responders during a nuclear catastrophe. An scFv would appear ideally suited for use in emergency scenarios as early evidence indicates it is available for administration by the subcutaneous route, has minimal toxicity, and is highly effective against GI-ARS lethality in well-established mouse models [18]. Here we explore in detail parameters of delivery that provide important information regarding future steps necessary for development of anti-ceramide 6B5 scFv (using a humanized version known as CX-01, a compound under development by Ceramedix Inc., a company that has licensed this technology) as an effective MRC of GI-ARS lethality.
Materials and Methods
Materials.
CX-01 (Lot # TP40533F), a humanized variant of anti-ceramide 6B5 [18], was provided by Ceramedix Holdings LLC at a concentration of 5.5mg/ml in HEPES buffer.
Radiation source.
Radiation was delivered to C57BL/6J mice (The Jackson Lab #000664) using a Shepherd Mark-I unit (Model 68, SN643) operating a 137Cs source at a dose rate of 1.48 Gy/min. The dose rate was established by Memorial Sloan-Kettering Cancer Center dedicated dosimetrists using a calibrated A12 ion chamber placed at the center of the irradiator turntable. The exposure rate was converted to dose rate to muscle in free space using the f-factor, 0.96 cGy/R. Output rates were adjusted for the decay of 137Cs (half-life of 30 years), on a 6-monthly basis. Original measurements, made at the time of commissioning, have been validated, most recently in 2015 and 2020. For prophylactic studies, pre-treatment with CX-01 was at 30 to 270 mins prior to irradiation, as indicated.
Survival of mice after whole body irradiation.
Actuarial survival of irradiated 8-12-week-old mice was calculated by the product limit Kaplan-Meier method [29]. Bone marrow cells obtained from male or female mice, harvested from the femur and tibia of C57BL/6J littermates, were washed, resuspended in culture medium, and at 20 hours post irradiation injected via tail vein (5x106 marrow cells/mouse) into sex-matched animals. Terminally sick animals displaying an agonal breathing pattern were sacrificed by hypercapnia asphyxiation. Note that commercial C57BL/6J male mice were subjected to the LD90 dose of 15 Gy for the GI-ARS as published [18], whereas in most experiments female mice were subject to the LD90 dose of 14.62 Gy.
Quantification of apoptosis.
Endothelial cell apoptosis was quantified in vivo in the small intestinal lamina propria following double staining with TUNEL, to detect apoptotic cells, and the endothelial cell surface marker MECA-32, as published by us [16, 30]. Briefly, mice were sacrificed at the indicated times post irradiation by CO2 asphyxiation and proximal jejunum at 10 cm from the Ligament of Treitz was fixed in 4% paraformaldehyde, embedded in paraffin, and 5-μm circumferential sections were stained sequentially with TUNEL assay and monoclonal antibody MECA-32. Apoptotic endothelial cells display a brown TUNEL positive nuclear signal surrounded by a dark blue plasma membrane signal indicative of MECA-32 staining. Data (mean ± SD) are derived from 150-200 imaged fields (40x) across 5-10 mice per group collated from 2 independent experiments.
Statistical analysis:
Statistical analyses of grouped data was performed using GraphPad Prism 8.0. For endothelial apoptosis experiments, unpaired t-tests were employed to evaluate statistical significance of differences, and 2-way ANOVA regression models were used to examine the difference between male and female mice. For animal survival studies the Kaplan-Meier method was used to estimate survival rates, and 2-way ANOVA (when survival was evaluated as binary outcome within 90 days) or log-rank test (when survival was evaluated as time-to-event data) was carried out for statistical comparison between sex or among various groups in terms of dose or timing. We considered p-values of less than 0.05 to be statistically significant and p > 0.05 not significant.
Results
Determination of the optimal anti-ceramide CX-01 prophylactic dose
Our previous data suggest that when irradiating 8-12-week-old C57BL/6J male mice with 15 Gy, the 90% lethal dose (LD90) for the GI-ARS in this mouse strain, the optimal protective dose of CX-01 against GI-ARS lethality is approximately 100 μg CX-01/mouse [18]. Here we perform full dose profiling from 25-200 μg per 8-12-week-old male and female mice administered in 25 μg increments to formally detail the optimal protective doses of CX-01, examining endothelial cell apoptosis at 6 hours post 15 Gy and Kaplan Meier Survival, as published [16]. For these initial studies, anti-ceramide CX-01 was delivered as prophylaxis subcutaneously at 30 minutes prior to irradiation. Fig. 1 shows histologic sections that display typical endothelial cell apoptosis in irradiated villi double stained with TUNEL and MECA-32, respectively, and counterstained with hematoxylin. Apoptotic endothelial cells (arrows) manifest a red-brown nuclear TUNEL signal surrounded by a blue-black membrane MECA-32-stained perimeter. Apoptotic endothelial cells in male mice exhibit an inverse profile relative to CX-01 concentration (Fig. 2A) with as little as 50 μg CX-01/mouse being effective, and a maximal effect achieved with 125 μg CX-01/mouse. Transformation of data yields an IC50 = 61.7 ± 5.7 μg CX-01/mouse (Fig. 2C).
As preliminary data indicated female mice might be more resistant to CX-01 radioprotection than male mice, the dose range was extended to 50-225 μg per 8-12-week-old female mice. Detailed dose range studies confirm that female mice display resistance to the inhibitory effect of anti-ceramide CX-01 compared with male mice with a minimally effective dose of 100 μg CX-01/female mouse and a maximal effect achieved with 150 μg CX-01/female mouse (Fig. 2B). Transformation of data yields a higher IC50 value for female than male mice = 106.8 ± 8.0 μg CX-01/female mouse (Fig. 2C; p<0.001 vs. male mice). Note, 8-12-week-old female mice weigh on average 20 g, whereas 8-12-week-old male mice weigh on average 25 g. Hence, the dose range used here in females is 2.5 - 11.25 mg/kg while the dose range in males is 1 - 8 mg/kg, and IC50 values are 5.3 mg/kg for females and 2.5 mg/kg for males, more than a 2-fold difference.
Based on these differences in CX-01 dosing, we fine-detailed the dose-range for Kaplan-Meier survival in female mice. We determined that 8-12-week-old C57BL/6J female mice were slightly more radiation sensitive than males with an LD90 dose of 14.62 Gy, a dose used throughout the rest of the studies reported here (Supplemental Fig. 1). Subsequent Kaplan Meier studies show, similar to the endothelial cell apoptosis data above, that female mice require higher doses of CX-01 to prevent GI-ARS lethality compared with male mice (Fig. 3A, B). As compared with endothelial cell apoptosis there was more variability in the protective effect provided by CX-01 against GI-ARS lethality for both sexes. Data transformation (Fig. 3C) yielded IC50 values for protection against GI-ARS lethality of 47.0 ± 3.0 mg CX-01/8-12-week-old male mice versus 159.1 ± 17.4 mg CX-01/8-12-week-old female mice (p=0.0199).
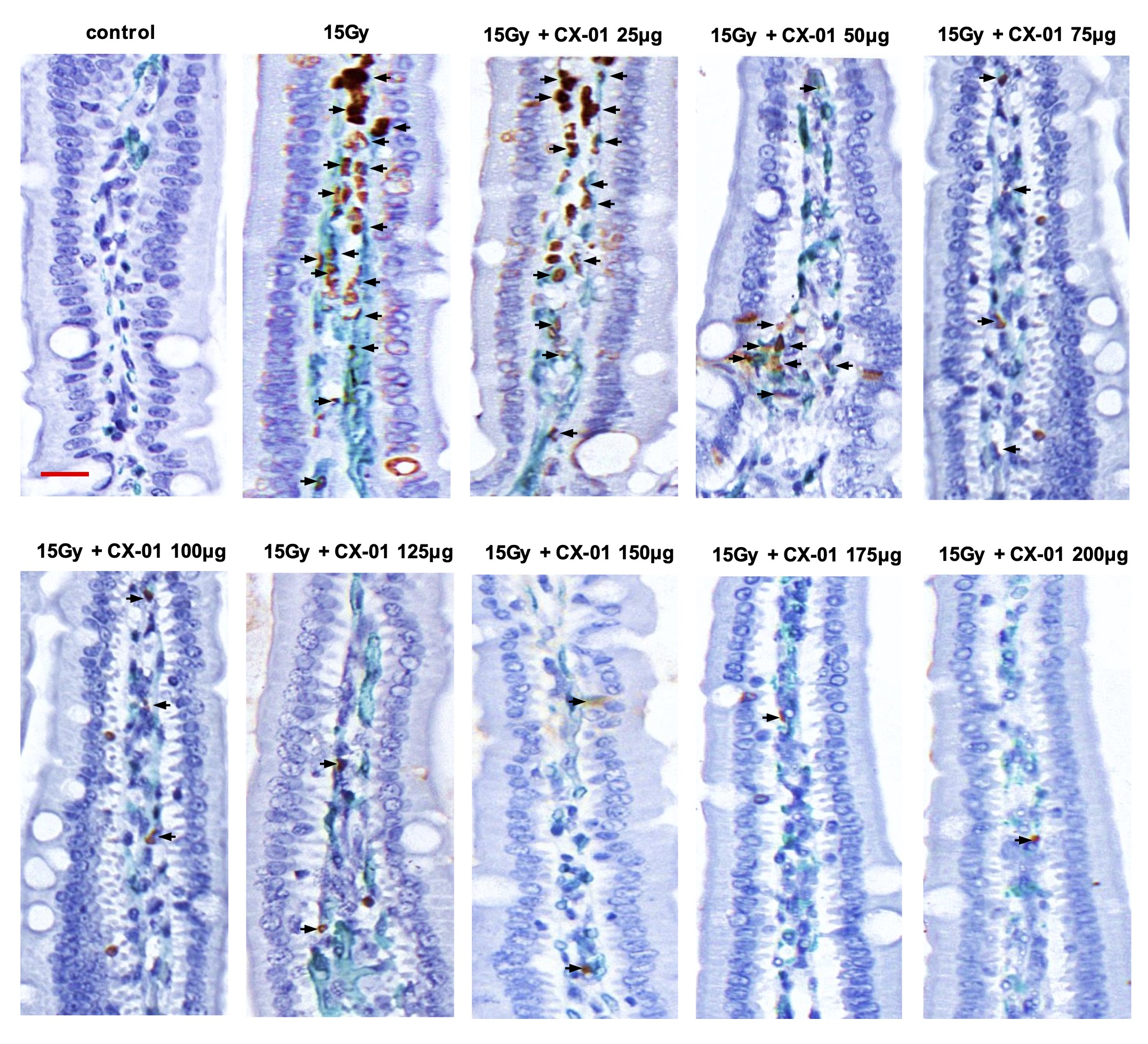
Fig. 1: CX-01 prophylaxis dose-dependently inhibits radiation-induced small intestinal endothelial cell apoptosis. 8-10-week-old C57BL/6J male mice were administrated CX-01 via s.c. injection at 30 min prior to 15Gy WBI with full dose profiling from 25-200 g CX-01/mouse. At 6 h post irradiation mice were sacrificed by CO2 asphyxiation and proximal jejunal circumferences at 10 cm from the Ligament of Treitz were prepared. Representative bright field images (40x) of 5-μm thick sections display villus endothelial cells undergoing apoptosis as determined by double staining for the endothelial cell surface marker MECA-32 (dark blue plasma membrane signal) and TUNEL (brown nuclear apoptotic signal), respectively. Normal nuclei (purple) are counterstained using hematoxylin. Scale bar: 20 μm.
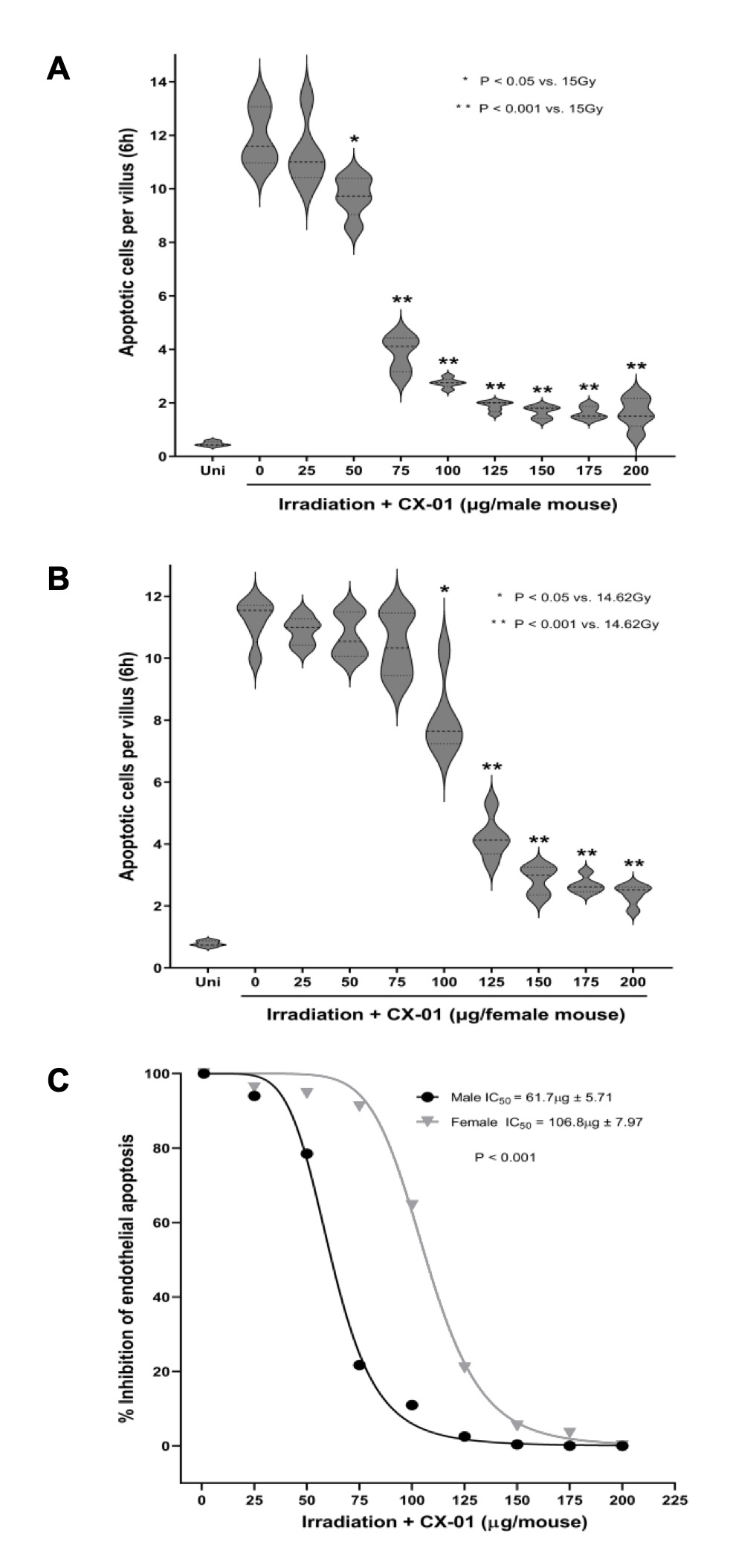
Fig. 2: Quantitation of dose dependent CX-01 prophylaxis of radiation-induced small intestinal endothelial apoptosis. (A) CX-01 was administered to C57BL/6J male mice s.c. at 30 min prior to 15Gy WBI with full CX-01 dose profiling from 25-200 μg CX-01/mouse. Endothelial apoptosis was identified at 6 h post irradiation by microscopic detection of TUNEL/MECA-32 double-positive endothelial cells as in Fig. 1. Data (mean ± SD) represent apoptotic endothelial cells/villus unit collated from 5 male mice/group, analyzing approximately 150-200 imaged fields. Unpaired t-test was employed to evaluate statistical significance of differences. (B) CX-01 was administered to C57BL/6J female mice s.c. at 30 min prior to 14.62Gy WBI with full dose profiling from 25-200 μg CX-01/mouse. Endothelial apoptosis was identified as in (A). (C) Transformed data depict female mice as more resistant to CX-01 prophylaxis of radiation-induced apoptosis compared with age-matched male mice. 2-way ANOVA was carried out for statistical comparison of male and female IC50 values.
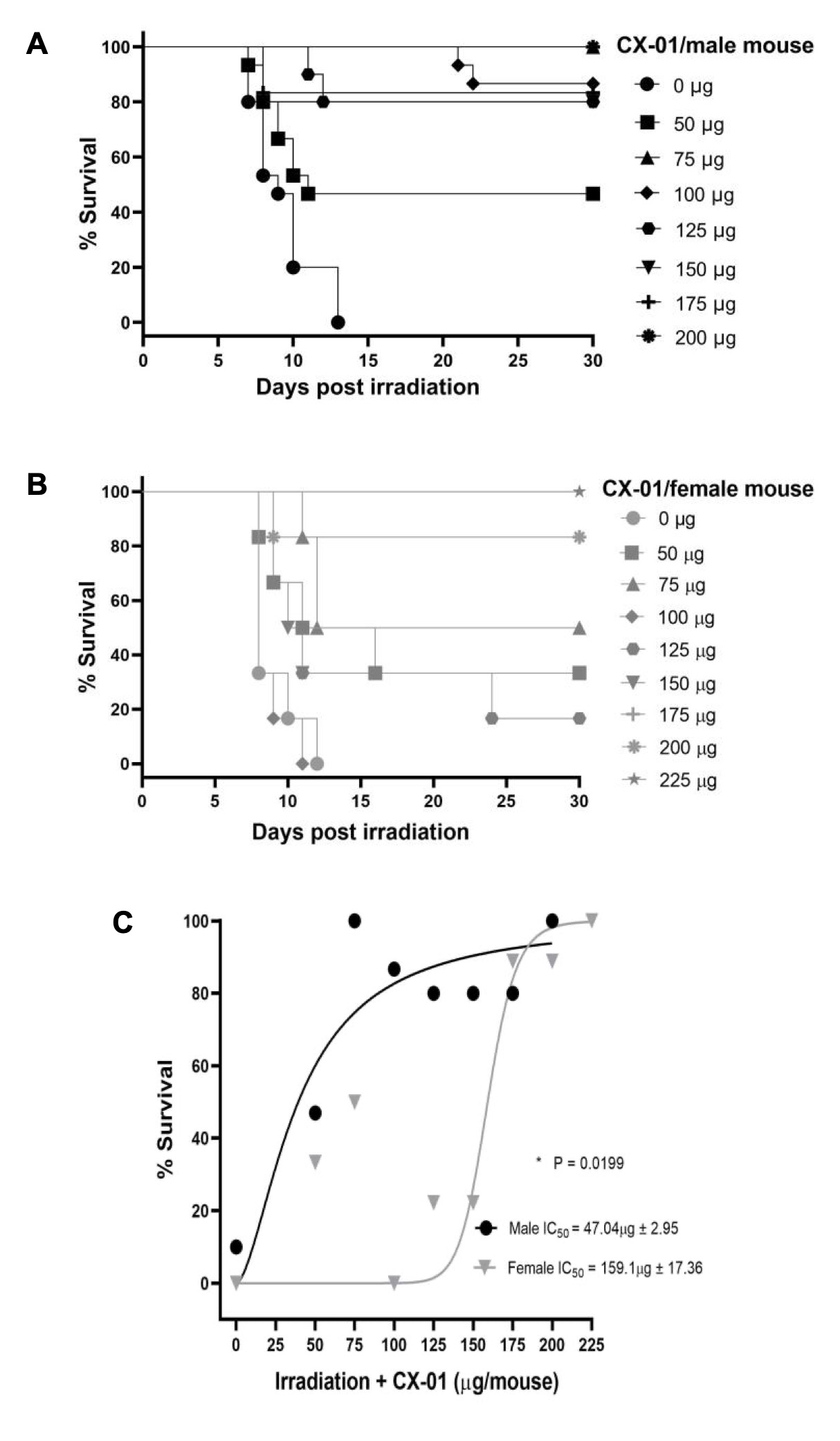
Fig. 3: Dose dependence of CX-01 radiation prophylaxis of Kaplan Meier survival from GI-ARS lethality. (A) CX-01 was administered s.c. at 30 min prior to 15Gy WBI with full dose profiling from 50-200 g CX-01/male mouse. (B) CX-01 was administered at 30 min prior to 14.62Gy WBI with full dose profiling from 50-225 g CX-01/female mouse. (C) Data transformation revealed for male mice IC50 = 47.04 g CX-01 and for female mice the IC50 = 159.1 g CX-01 (p = 0.0199). Mice were monitored for survival for 90 days. Bone marrow cells (5x106 cells/mouse) transplanted at 20 hours post irradiation injected via tail vein into animals. 15 mice were used in each study group. Kaplan-Meier method was used to estimate survival rates and 2-way ANOVA was carried out for statistical comparison of male and female IC50 values.

Determination of the optimal anti-ceramide CX-01 prophylactic schedule
Preliminary data indicate that anti-ceramide CX-01 can be delivered effectively as prophylaxis at any time within 1-hour preceding radiation exposure. Based on dose dependence studies performed above, formal scheduling studies were performed using a slightly more than maximally-effective dose of 150 μg for male mice and 200 μg for females, delivering CX-01 in ½ hour increments in progressively longer intervals prior to irradiation, evaluating the two GI-ARS assays described above. Fig. 4 shows that the optimal window of time for administration of anti-ceramide CX-01 pre-treatment to provide maximal protection from endothelial cell apoptosis in the small intestinal lamina propria of 8-12-week-old male C57BL/6J mice is within 120 minutes preceding radiation exposure in both male and female mice. Timing of CX-01 administration for achieving 50% protection in male mice is 156.2 minutes and in female mice is 128.79 minutes, a difference that is statistically significant (p=0.0309). Complementary studies examining Kaplan Meier survival (Fig. 5) show the optimal window of time for administration of anti-ceramide CX-01 to provide maximal prophylaxis from GI-ARS lethality in 8-12-week-old C57BL/6J mice is within 90 minutes in both male and female mice. Timing of CX-01 administration for achieving 50% survival in male mice is 128.2 minutes and in female mice is 121.9 minutes (p=0.169).
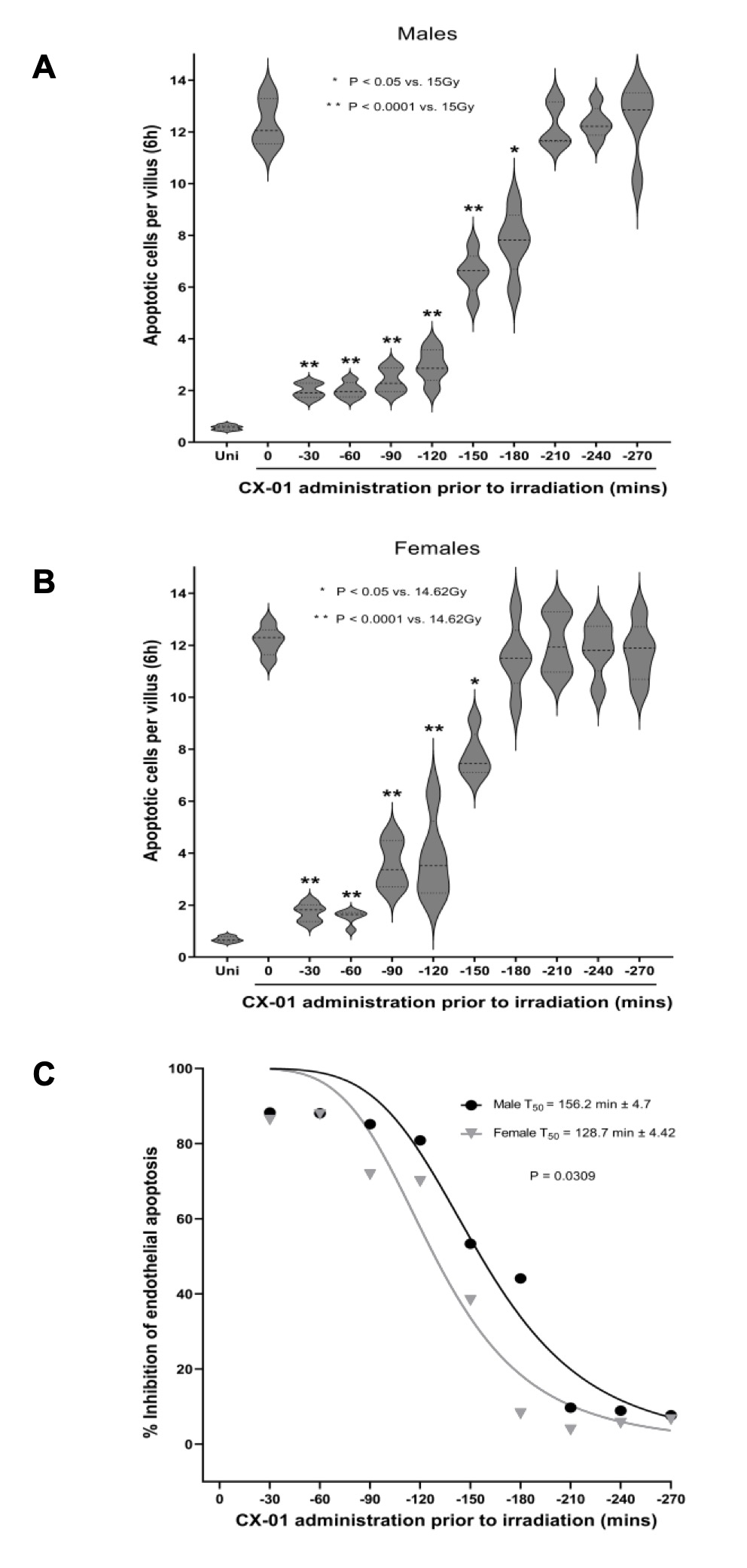
Fig. 4: Time dependence of CX-01 prophylaxis of radiation-induced endothelial cell apoptosis. (A) CX-01 was administered in half-hour increments preceding 15Gy (at -30 to -270 min) using the optimal dose of 150 g CX-01/male mouse. Endothelial apoptosis was quantified at 6 h post-irradiation by TUNEL/MECA-32 double staining as in Fig. 2. Data (mean ± SD) represent apoptotic endothelial cells/villus unit collated from 5 male mice/group, analyzing approximately 150-200 imaged fields. Unpaired t-test was employed to evaluate statistical significance of differences. (B) CX-01 was administered in half-hour increments preceding 14.62Gy (at -30 to -270 min) using the optimal dose of 200 g CX-01/female mouse. Endothelial apoptosis was quantified as in (A). (C) Transformed data depict time-dependent inhibition of radiation-induced endothelial apoptosis in intestines by CX-01. Timing of CX-01 administration for achieving 50% protection in male mice = 156.2 minutes and in females = 128.7 minutes (p = 0.0309). 2-way ANOVA was carried out for statistical comparison of male and female T50 values.
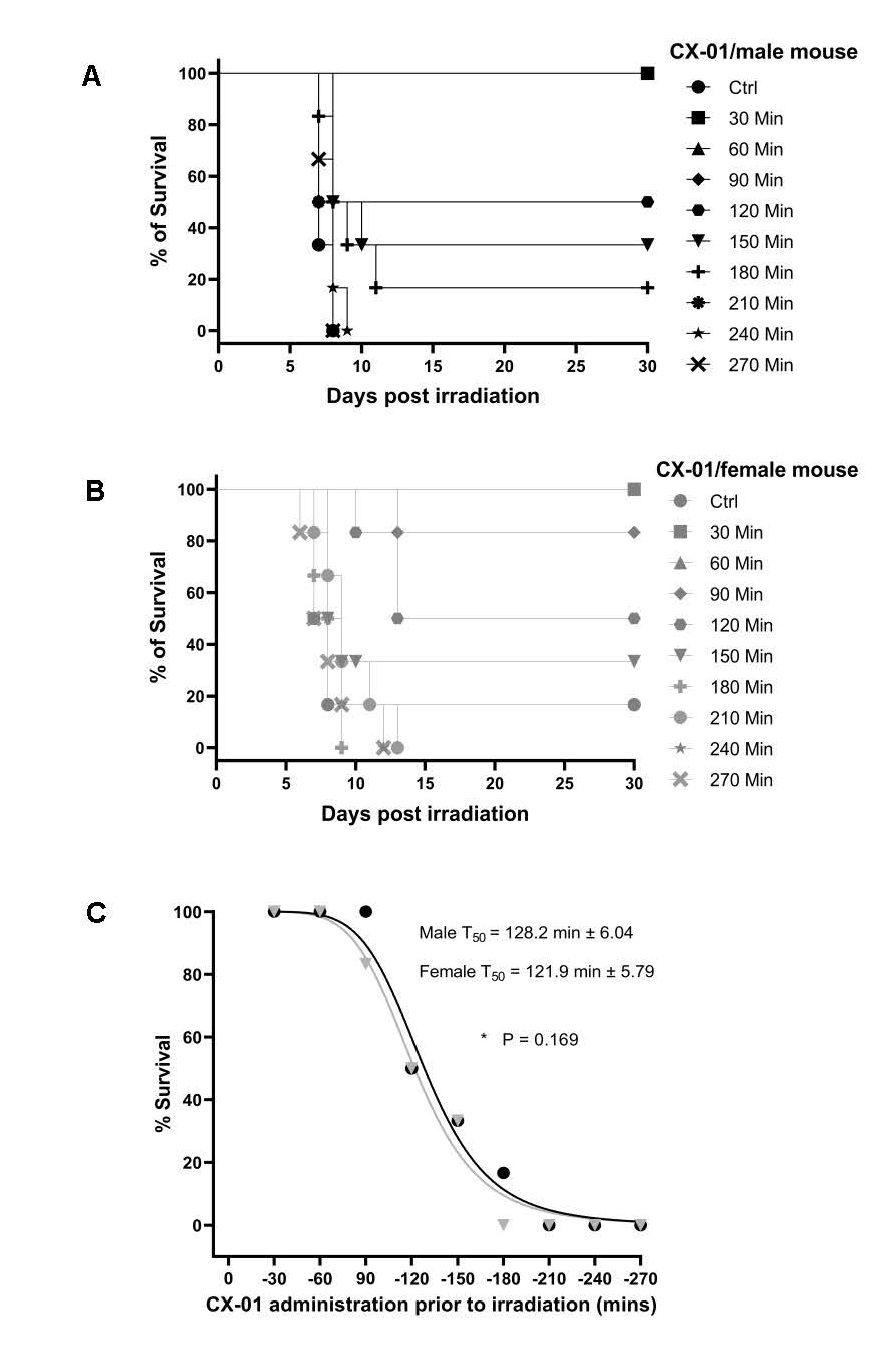
Fig. 5: Time dependence of CX-01 radiation prophylaxis of Kaplan Meier survival. (A) CX-01 was administered in half-hour increments preceding 15Gy (at -30 to -270 min) using the optimal dose of 150 g CX-01/25 male mouse. (B) CX-01 was administered in half-hour increments preceding 14.62Gy (at -30 to -270 min) using optimal dose 200 μg CX-01/female mouse. (C) Transformed data show the time of CX-01 pre-treatment for achieving 50% survival in male mice = 128.2 minutes and in females = 121.9 minutes (p = 0.169). Mice were monitored for 90 days to determine survival. Bone marrow cells (5x106 cells/mouse) transplanted at 20 hours post irradiation injected via tail vein into animals.15 mice were used in each study group. Kaplan-Meier method was used to estimate survival rates and 2-way ANOVA was carried out for statistical comparison of male and female T50 values.

Determination of the optimal anti-ceramide CX-01 route of administration
Preliminary investigations indicate that anti-ceramide CX-01 might be similarly effective as prophylaxis when delivered by subcutaneous or intramuscular routes. Fig. 6 formally shows that anti-ceramide CX-01, when delivered at 30 minutes prior to 15 Gy irradiation, is equally effective by the intramuscular or subcutaneous route of administration in preventing radiation-induced intestinal damage from endothelial cell apoptosis, examined at 6 hours post radiation, in both male and female mice. Complementary studies examining Kaplan Meier survival show 80% survival of mice with either the intramuscular or subcutaneous route of administration. These latter survival data are thus highly consistent with the endothelial apoptosis studies.
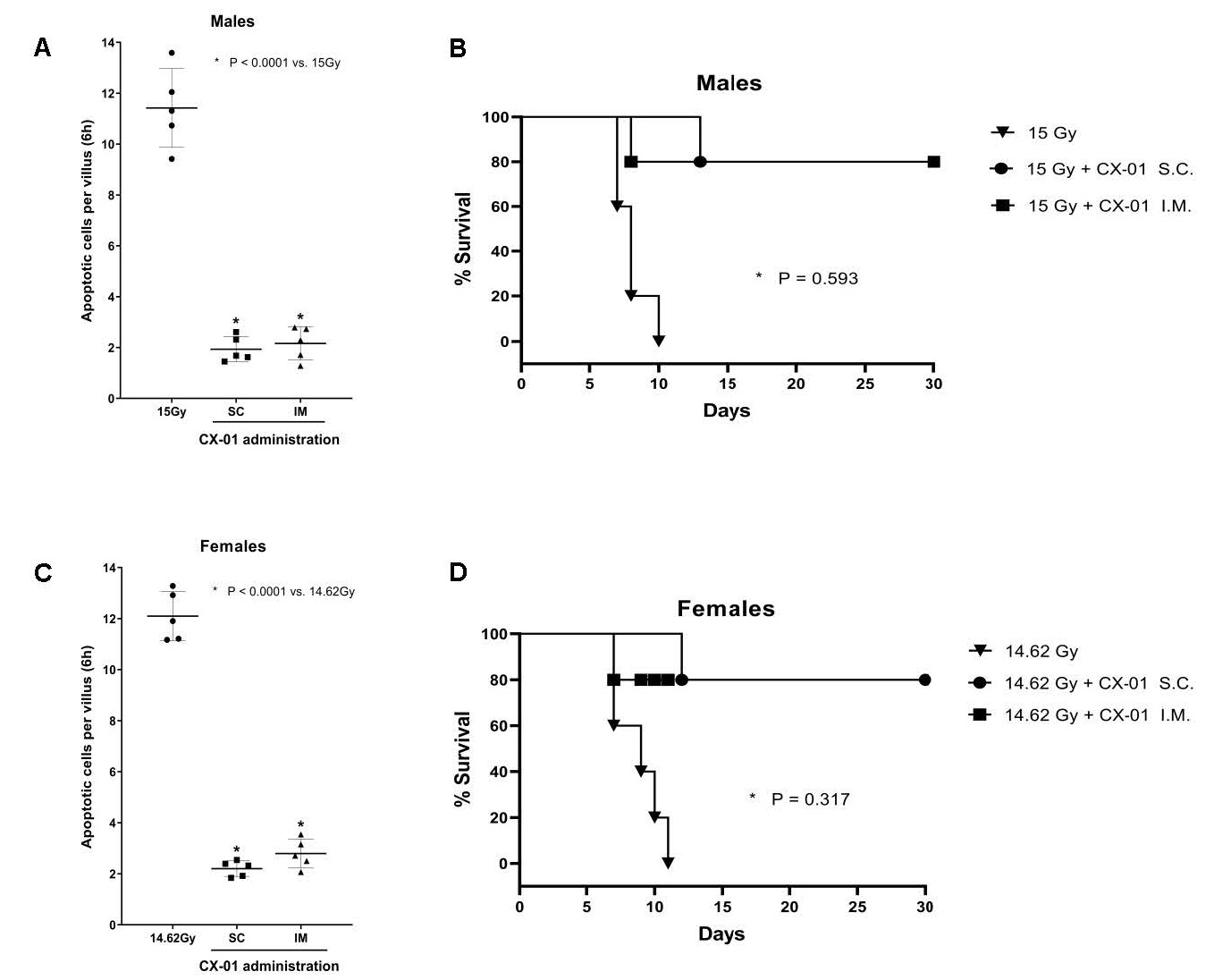
Fig. 6: Determination of CX-01 optimal route of administration. (A) CX-01 was administered at 30 min via s.c. and i.m. routes, respectively, prior to 15Gy WBI using the optimal dose of 150 g/male mouse. Endothelial apoptosis was identified at 6 h post irradiation by microscopic detection of TUNEL/MECA-32 double-positive endothelial cells. Data (mean ± SD) represent apoptotic endothelial cells/villus unit collated from 5 male mice/group, analyzing approximately 150-200 imaged fields. (B) Kaplan Meier studies to determine CX-01 optimal route of administration in male mice (15 mice per group) for protection from GI-ARS lethality. (C) CX-01 was administered at 30 min via s.c. and i.m. routes, respectively, prior to 14.62Gy WBI using the optimal dose of 200 g CX-01/female mouse. Endothelial apoptosis was quantified as in (A). Data (mean ± SD) represent apoptotic endothelial cells/villus unit collated from 5 female male mice/group, analyzing approximately 150-200 imaged fields. (D) Kaplan Meier studies to determine CX-01 optimal route of administration in female mice (15 mice per group) for protection from GI-ARS lethality. Unpaired t-tests were employed to evaluate statistical significance of differences in (A, C). Log-rank tests were carried out to evaluate statistical significance in (B, D).
Determination of whether increasing CX-01 dose to supra-optimal levels will extend the period of effectiveness
A study performed by the Radiation Countermeasures Program at NIAID was conducted at SRI International to determine the safety of 6B5 scFv as a single dose administered subcutaneously to female C57BL/6J mice (SRI Study R050-18). No test-article related effects were observed for clinical observations, body weights, clinical pathology, macroscopic or microscopic evaluations. Results from this study showed that the maximum tolerated dose (MTD) and the ‘no observed adverse effect level (or NOAEL)’ is at least ~832 μg/8-10-week-old female mouse (or 33.3 mg/kg) for 6B5 scFv, which is >4X the optimal dose of 200 μg/8-10-week-old female mouse reported here. These findings are consistent with the biology, which indicates absent significant membrane stress, this system is in the “off” state, and hence there is almost no available ceramide antigen on the surface of an endothelial cell [14, 25-28]. Fig. 7A, C shows that delivery of 5X the maximally-effective CX-01 dose for each sex, as described above, is most effective in preventing endothelial apoptosis when delivered at -30 to -120 minutes preceding irradiation, and equally effective as the 1X dose (p=0.151 in male, p=0.059 in female). We conclude that increasing the dose to supra-optimal 5X levels likely only marginally improves outcome when compared to the 1X maximal dose in both male and female mice. Complementary studies examining Kaplan Meier survival (Fig. 7B, D) show very similar data for 1X and 5X doses of CX-01 in protecting against GI-ARS lethality in both male and female mice (p=0.053 in male, p=0.346 in female), highly consistent with the endothelial apoptosis studies.
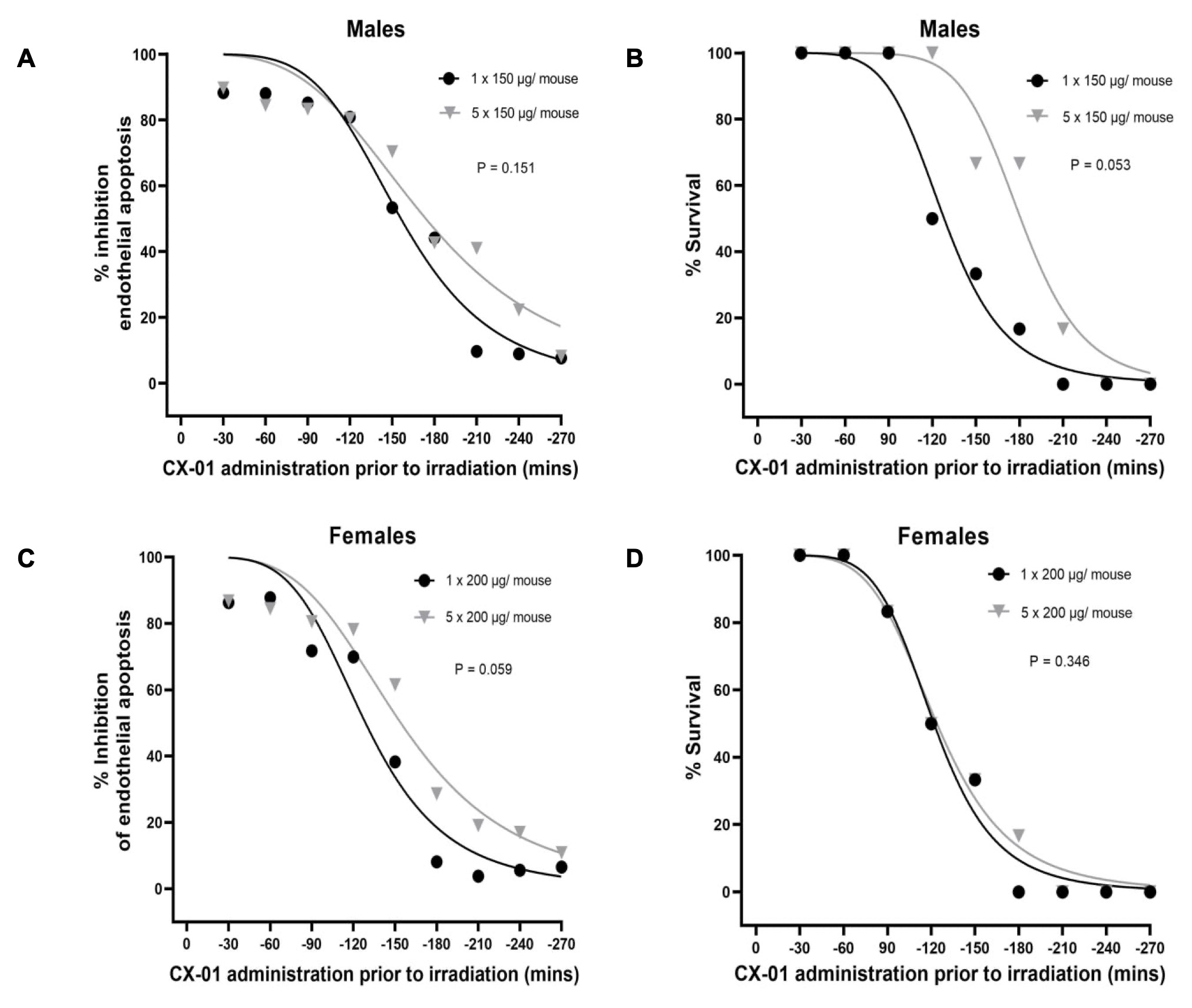
Fig. 7: Impact of 1 X and 5 X CX-01 doses on time dependence of radiation prophylaxis. (A) CX-01 was administered s.c. in half-hour increments preceding 15Gy (at -30 to -270 min) comparing the supra-optimal dose of 5x150 g CX-01/male mouse to the maximally effective dose of 150 g CX-01/male mouse. 5 male mice were used in each study group. Endothelial apoptosis was quantified as in Fig.s 1 and 2. Transformed data depict highly similar dose-dependent inhibitory profiles of radiation-induced endothelial apoptosis using 1X and 5 X CX-01 doses. (B) Kaplan Meier studies were performed as in A monitoring mice for 90 days. Timing of CX-01 administration for achieving 50% survival after 1 X dosing = 128.2 minutes and after 5 X dosing = 180.8 minutes (p = 0.43). 15 mice were used in each study group. (C) CX-01 was administered s.c. in half-hour increments preceding 14.62Gy (at -30 to -270 min) comparing the supra-optimal dose of 5x200 μg CX-01/female mouse to the maximally effective dose of 200 μg CX-01/female mouse. 5 female mice were used in each study group. Endothelial apoptosis was analyzed as in A. Transformed data depict highly similar dose-dependent inhibition of radiation-induced endothelial apoptosis in the small intestines of female mice by CX-01 1X and 5 X doses. (D) Kaplan Meier studies to determine time dependent CX-01 protection of female mice from GI-ARS lethality using 1X and 5 X doses were performed as in C. Survival was monitored at 90 days. Timing of CX-01 administration for achieving 50% survival after 1 X dosing = 121.9 minutes and after 5 X dosing = 123.9 minutes (p = 0.92). 15 mice were used in each study group. 2-way ANOVA was carried out for statistical comparisons in these studies.
Discussion
The current study is the first to detail the potential use of anti-ceramide scFv CX-01 as a radioprotector for first responders to a nuclear catastrophe, and demonstrates novel findings, some of which are unanticipated. Firstly, these studies show that female and male mice display similar levels of protection from small intestinal endothelial cell apoptosis, a critical mediator of GI-ARS morbidity and mortality, as well as similar levels of protection from radiation-induced lethality. Additionally, in both sexes subcutaneous and intramuscular routes of CX-01 administration are effective, optimal timing of CX-01 delivery is similar, and increasing dose is ineffective in prolonging radioprotection. While capability of peripheral delivery will ease drug administration under mass casualty conditions, human females may, based on the current data set in rodents, require significantly larger doses of CX-01 compared with males to obtain comparable protection from endothelial cell apoptosis and GI-ARS lethality. The reason for this difference is currently unknown. Fig. 8 displays an up-to-date schema that provides a rationale for use of CX-01 as an MRC for first responders to a nuclear catastrophe in the context of GI-ARS pathophysiology, as we now understand it.
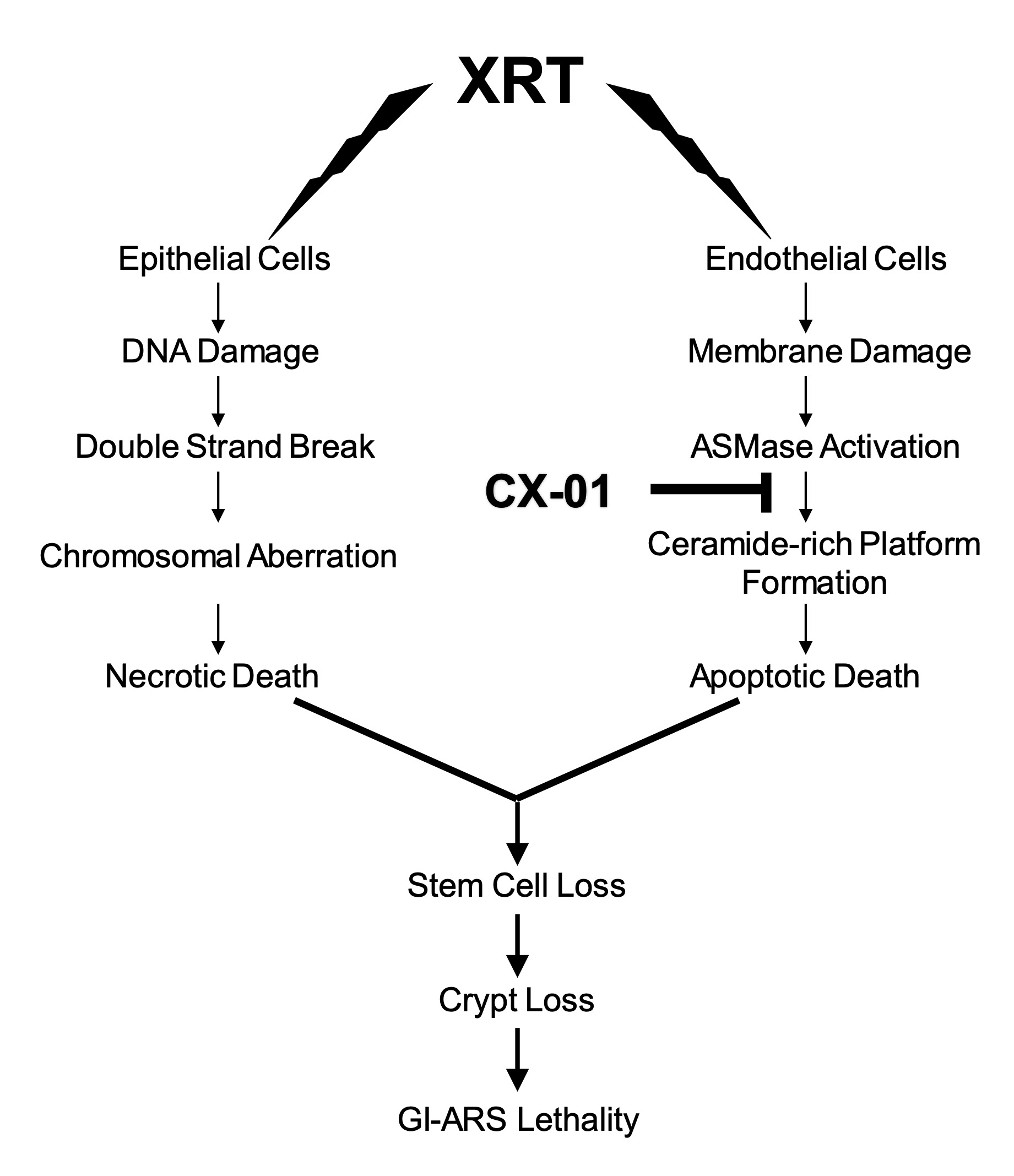
Fig. 8: Schematic mechanism of XRT-induced intestinal damage. Ultra-high dose ionizing radiation (XRT) simultaneously injures epithelial cell DNA and endothelial cell plasma membranes. Unrepaired double strand breaks degenerate into chromosomal aberrations which lead to epithelial cell necrotic death. Endothelial cells rapidly release large amounts of acid sphingomyelinase (ASMase) that hydrolyzes sphingomyelin preferentially concentrated in the outer endothelial plasma membrane to generate ceramide. Ceramide, due to unique biophysical properties, rapidly self-associates into a large macrodomain termed a ceramide-rich platform (CRP), which transmits an apoptotic signal. Concomitant epithelial and endothelial injury act synthetically to yield irreversible intestinal stem cell loss. Delivery of an anti-ceramide antibody CX-01 to neutralize the pro-apoptotic lipid ceramide on the GI endothelial cell surface can prevent CRP formation, abrogating endothelial apoptosis, protecting against crypt stem cell loss and GI-ARS lethality.
While anti-ceramide 6B5, the parental monoclonal Ab from which CX-01 was derived, was originally isolated as a murine IgG, and thereafter humanized and reduced in size to permit access via the subcutaneous and intramuscular routes, in so doing the half-life was shortened in mice from days to hours [18]. This property did not seem to impinge on use of CX-01 as an effective mitigator of ongoing endothelial apoptosis and ensuing GI-ARS lethality in the same C57BL/6J model used in the current study. However, the short half-life might be an impediment for development of CX-01 as potential prophylaxis for first responders, as shown in the current study. While it may be possible to use CX-01 as it is currently designed with repeated injections, perhaps by using an auto-injector in a mass casualty setting, a more reasonable approach to this problem might be to increase half-life by increasing fragment size, while retaining complementarity-determining regions necessary for antigen recognition. In this context, our studies using 2A2 anti-ceramide Ab showed that a Fab fragment of 2A2 anti-ceramide Ab with a MW ~50 kDa (vs. 29 kDa for CX-01), retained bioeffectiveness in C57BL/6 mice (Rotolo J and Kolesnick R, unpublished). Furthermore, preliminary data indicate that even CX-01, when re-engineered to contain a full-length Fc, retains bioeffectiveness when delivered subcutaneously or intramuscularly (Kumar, P and Kolesnick, R, unpublished). Hence, re-design of CX-01 to be more user friendly in battlefield conditions might be warranted.
A pilot study funded by NIAID under a Nonclinical Evaluation Agreement with Ceramedix, conducted by Stanford Research International (SRI) at Citox Labs (now Charles River Laboratories) evaluated PK and efficacy of HIS-tagged CX-01 in non-human primates (rhesus macaques), with and without irradiation. Our MSK laboratory was under sub-contract for these studies. Data (R Kolesnick et al., unpublished) from the GI tract and lungs of these animals showed the following findings: 1) The time course and magnitude of the endothelial apoptotic response in the NHP GI tract after a GI-ARS LD50 dose of 11.5 Gy with 5% partial body irradiation are highly similar between mice and monkeys; 2) Allometrically scaled CX-01 was effective as a protector and dose-dependently as a mitigator of GI endothelial cell apoptosis; 3) Similar kinetics and CX-01 protection/mitigation of endothelial cell apoptosis were detected in rhesus lungs when compared with GI tract; 4) There were no differences between the sexes (although this study was limited to 1 male and female per time point). These data, which are currently in process of being written up for publication, provide cross-species validation of the rationale for pursuing development of CX-01 as an MRC and support the notion of its redesign, based on information from the current studies, of CX-01 for use as prophylaxis for first responders to a nuclear disaster.
Acknowledgements
This work was supported by funds provided by National Institute of Allergy and Infectious Diseases, Joint Warfighter Medical Research Program from the United States Department of Defense and The Center for Experimental Therapeutics and Molecular Cytology Core at Memorial Sloan Kettering Cancer.
Author contributions
JC, PN, RF and TB performed experiments, acquired, and analyzed data; JC and RK wrote the manuscript; ZF and RK provided overall scientific direction and supervision.
Funding Sources
This work was supported by funds provided by the US Army Medical Research and Development Command under Contract No. W81XWH20C0042 to Ceramedix Inc. on which MSK is a sub-contractor. This research was also funded through a NIH/National Cancer Institute Cancer Center Support Core Grant P30 CA008748 to RK.
Statement of Ethics
Mice were housed at the Research Animal Resource Center of Memorial Sloan-Kettering Cancer Center. In conducting research using animals, the investigator(s) adhered to the Animal Welfare Act Regulations and other Federal statutes relating to animals and experiments involving animals and the principles set forth in the current version of the Guide for Care and Use of Laboratory Animals, National Research Council.
Disclosure Statement
RK holds the following patents: US7195775B1, US7850984B2, and US10052387B2, US10414533B2, US20140205543A1, US8562993B2, US9592238B2, US10450385B2, US20150216971A1, US20170335014A1, US20190389970A1, and US20190046538A1; RK and ZF hold the following patents: US20170333413A1 and US20180015183A1); ZF holds the following patent: US10413533B2. RK and ZF are co-founders of Ceramedix Holding LLC.
References
| 1 | DiCarlo AL: Scientific research and product development in the United States to address injuries from a radiation public health emergency. J Radiat Res 2021;62:752-763.
https://doi.org/10.1093/jrr/rrab064 |
| 2 | DiCarlo AL, Homer MJ, Coleman CN: United States medical preparedness for nuclear and radiological emergencies. J Radiol Prot 2021;4:5.
https://doi.org/10.1088/1361-6498/ac0d3f |
| 3 | DiCarlo AL, Cassatt DR, Dowling WE, Esker JL, Hewitt JA, Selivanova O, Williams MS, Price PW: Challenges and Benefits of Repurposing Products for Use during a Radiation Public Health Emergency: Lessons Learned from Biological Threats and other Disease Treatments. Radiat Res 2018;190:659-676.
https://doi.org/10.1667/RR15137.1 |
| 4 | Cassatt DR, Gorovets A, Karimi-Shah B, Roberts R, Price PW, Satyamitra MM, Todd N, Wang SJ, Marzella L: A Trans-Agency Workshop on the Pathophysiology of Radiation-Induced Lung Injury. Radiat Res 2022;197:415-433.
https://doi.org/10.1667/RADE-21-00127.1 |
| 5 | Hendry JH, Potten CS, Roberts NP: The gastrointestinal syndrome and mucosal clonogenic cells: relationships between target cell sensitivities, LD50 and cell survival, and their modification by antibiotics. Radiat Res 1983;96:100-112.
https://doi.org/10.2307/3576169 |
| 6 | Hendry JH, Roberts SA, Potten CS: The clonogen content of murine intestinal crypts: dependence on radiation dose used in its determination. Radiat Res 1992;132:115-119.
https://doi.org/10.2307/3578342 |
| 7 | Potten CS: A comprehensive study of the radiobiological response of the murine (BDF1) small intestine. Int J Radiat Biol 1990;58:925-973.
https://doi.org/10.1080/09553009014552281 |
| 8 | Hua G, Wang C, Pan Y, Zeng Z, Lee SG, Martin ML, Haimovitz-Friedman A, Fuks Z, Paty PB, Kolesnick R: Distinct Levels of Radioresistance in Lgr5(+) Colonic Epithelial Stem Cells versus Lgr5(+) Small Intestinal Stem Cells. Cancer Res 2017;77:2124-2133.
https://doi.org/10.1158/0008-5472.CAN-15-2870 |
| 9 | Martin ML, Adileh M, Hsu KS, Hua G, Lee SG, Li C, Fuller JD, Rotolo JA, Bodo S, Klingler S, Haimovitz-Friedman A, Deasy JO, Fuks Z, Paty PB, Kolesnick RN: Organoids Reveal That Inherent Radiosensitivity of Small and Large Intestinal Stem Cells Determines Organ Sensitivity. Cancer Res 2020;80:1219-1227. DO
https://doi.org/10.1158/0008-5472.CAN-19-0312 |
| 10 | Barker N, van Es JH, Kuipers J, Kujala P, van den Born M, Cozijnsen M, Haegebarth A, Korving J, Begthel H, Peters PJ, Clevers H: Identification of stem cells in small intestine and colon by marker gene Lgr5. Nature 2007;449:1003-1007.
https://doi.org/10.1038/nature06196 |
| 11 | Barker N, Ridgway RA, van Es JH, van de Wetering M, Begthel H, van den Born M, Danenberg E, Clarke AR, Sansom OJ, Clevers H: Crypt stem cells as the cells-of-origin of intestinal cancer. Nature 2009;457:608-611.
https://doi.org/10.1038/nature07602 |
| 12 | Sato T, Vries RG, Snippert HJ, van de Wetering M, Barker N, Stange DE, van Es JH, Abo A, Kujala P, Peters PJ, Clevers H: Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymal niche. Nature 2009;459:262-265.
https://doi.org/10.1038/nature07935 |
| 13 | Santana P, Pena LA, Haimovitz-Friedman A, Martin S, Green D, McLoughlin M, Cordon-Cardo C, Schuchman EH, Fuks Z, Kolesnick R: Acid sphingomyelinase-deficient human lymphoblasts and mice are defective in radiation-induced apoptosis. Cell 1996;86:189-199.
https://doi.org/10.1016/S0092-8674(00)80091-4 |
| 14 | Paris F, Fuks Z, Kang A, Capodieci P, Juan G, Ehleiter D, Haimovitz-Friedman A, Cordon-Cardo C, Kolesnick R: Endothelial apoptosis as the primary lesion initiating intestinal radiation damage in mice. Science 2001;293:293-297.
https://doi.org/10.1126/science.1060191 |
| 15 | Rotolo JA, Kolesnick R, Fuks Z: Timing of lethality from gastrointestinal syndrome in mice revisited. Int J Radiat Oncol Biol Phys 2009;73:6-8.
https://doi.org/10.1016/j.ijrobp.2008.09.009 |
| 16 | Rotolo J, Stancevic B, Zhang J, Hua G, Fuller J, Yin X, Haimovitz-Friedman A, Kim K, Qian M, Cardo-Vila M, Fuks Z, Pasqualini R, Arap W, Kolesnick R: Anti-ceramide antibody prevents the radiation gastrointestinal syndrome in mice. J Clin Invest 2012;122:1786-1790.
https://doi.org/10.1172/JCI59920 |
| 17 | Stancevic B, Kolesnick R: Ceramide-rich platforms in transmembrane signaling. FEBS Lett 2010;584:1728-1740.
https://doi.org/10.1016/j.febslet.2010.02.026 |
| 18 | Rotolo JA, Fong CS, Bodo S, Nagesh PK, Fuller J, Sharma T, Piersigilli A, Zhang Z, Fuks Z, Singh VK, Kolesnick R: Anti-ceramide single-chain variable fragment mitigates radiation GI syndrome mortality independent of DNA repair. JCI Insight 2021;6:8.
https://doi.org/10.1172/jci.insight.145380 |
| 19 | Rojavin Y, Seamon MJ, Tripathi RS, Papadimos TJ, Galwankar S, Kman N, Cipolla J, Grossman MD, Marchigiani R, Stawicki SP: Civilian nuclear incidents: An overview of historical, medical, and scientific aspects. J Emerg Trauma Shock 2011;4:260-272.
https://doi.org/10.4103/0974-2700.82219 |
| 20 | Runge JW, Buddemeier BR: Explosions and radioactive material: a primer for responders. Prehosp Emerg Care 2009;13:407-419.
https://doi.org/10.1080/10903120902935371 |
| 21 | Musolino SV, Harper FT: Emergency response guidance for the first 48 hours after the outdoor detonation of an explosive radiological dispersal device. Health Phys 2006;90:377-385.
https://doi.org/10.1097/01.HP.0000196111.16261.ed |
| 22 | Sproull M, Rebmann T, Turner A, Charney R, Petricoin E, Koblentz GD, Kennedy WG: Computational modeling of first responders' willingness to accept radiation exposure during radiological or nuclear events. Am J Disaster Med 2022;17:101-115.
https://doi.org/10.5055/ajdm.2022.0424 |
| 23 | Rebmann T, Charney RL, Loux TM, Turner JA, Nguyen D: Firefighters' and Emergency Medical Service Personnel's Knowledge and Training on Radiation Exposures and Safety: Results from a Survey. Health Secur 2019;17:393-402.
https://doi.org/10.1089/hs.2019.0086 |
| 24 | Blumenthal DJ, Bader JL, Christensen D, Koerner J, Cuellar J, Hinds S, Crapo J, Glassman E, Potter AB, Singletary L: A sustainable training strategy for improving health care following a catastrophic radiological or nuclear incident. Prehosp Disaster Med 2014;29:80-86.
https://doi.org/10.1017/S1049023X1400003X |
| 25 | Grassme H, Jendrossek V, Riehle A, von Kurthy G, Berger J, Schwarz H, Weller M, Kolesnick R, Gulbins E: Host defense against Pseudomonas aeruginosa requires ceramide-rich membrane rafts. Nat Med 2003;9:322-330.
https://doi.org/10.1038/nm823 |
| 26 | Perez GI, Jurisicova A, Matikainen T, Moriyama T, Kim MR, Takai Y, Pru JK, Kolesnick RN, Tilly JL: A central role for ceramide in the age-related acceleration of apoptosis in the female germline. FASEB J 2005;19:860-862.
https://doi.org/10.1096/fj.04-2903fje |
| 27 | Jacobi J, Garcia-Barros M, Rao S, Rotolo JA, Thompson C, Mizrachi A, Feldman R, Manova K, Bielawska A, Bielawska J, Fuks Z, Kolesnick R, Haimovitz-Friedman A: Targeting acid sphingomyelinase with anti-angiogenic chemotherapy. Cell Signal 2017;29:52-61.
https://doi.org/10.1016/j.cellsig.2016.09.010 |
| 28 | Ferranti CS, Cheng J, Thompson C, Zhang J, Rotolo JA, Buddaseth S, Fuks Z, Kolesnick RN: Fusion of lysosomes to plasma membrane initiates radiation-induced apoptosis. J Cell Biol 2020;219:4.
https://doi.org/10.1083/jcb.201903176 |
| 29 | Kaplan EL, Meier P: Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association 1958;53:457-481.
https://doi.org/10.1080/01621459.1958.10501452 |
| 30 | Garcia-Barros M, Paris F, Cordon-Cardo C, Lyden D, Rafii S, Haimovitz-Friedman A, Fuks Z, Kolesnick R: Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science 2003;300:1155-1159.
https://doi.org/10.1126/science.1082504 |